How to get inside?
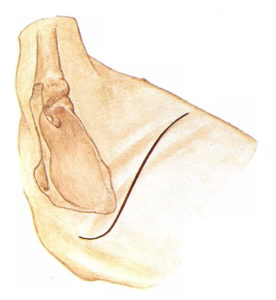
This was not a meaningful question until the 1990s. Up till then the only route in was by an open thoracotomy. (from thorax, chest, and -otomy, to open) The figure illustrates. A cut in the skin and muscles is parallel to the ribs which are spread apart. This opens the chest up and provides unhindered access to the chest contents. Great for the surgeon; less so for the patient. All the cutting and spreading of the ribs (and the nerves which accompany them) results in considerable pain after the operation.
In the 1990s an alternative emerged. Broadly called minimally invasive surgery and used to access several body cavities, for the chest it’s referred to as thoracoscopy. (from thorax and -oscopy, to look) Three to five small cuts are made in the skin and tubes, called ports, are put through them into the chest cavity. Operating instruments and a video camera are inserted through the ports. Muscle is not incised and ribs are not spread. The result is the same operation but less pain and a quicker recovery for the patient. Special training for the surgeon is required to master this technique but it is quickly penetrating thoracic surgery and, I’m sure, will soon be the standard way to perform most chest operations.
Also available is so-called robotic surgery but this is a misnomer. The thoracoscopic instruments are attached to mechanical arms which are manipulated by a thoracic surgeon seated at a computer console. The incisions in the patient are identical to those for the minimally invasive approach. This system has some theoretical advantages but is expensive and has not been shown to improve patient outcomes so its future use is uncertain.
Which of these three is best? The thoracotomy approach has been the gold standard and is still preferred by the majority of surgeons. However, the patient experiences significant pain afterwards and is usually in the hospital five or more days. The minimally invasive technique is associated with less pain, less time in the hospital, quicker recovery and is preferred by younger surgeons. It will likely become the most commonly used approach as older surgeons (like me) are replaced by those more recently trained. The robotic set-up has some technical benefits but is expensive and provides results essentially identical to those by the minimally invasive approach.
